Anatomy and Physiology (A&P) of the Upper Airway
The airway begins at the tip of the nose and the lips and ends at the alveolocapillary membrane, through which gas exchange takes place between the air sacs of the lung (the alveoli) and the lung’s capillary network. The airway consists of chambers and pipes, which conduct air with its 21% oxygen content to the alveoli and carry away the waste carbon dioxide that diffuses from the blood into the alveoli.
In this first aid blog post we will look closer at the anatomy of the upper airway.
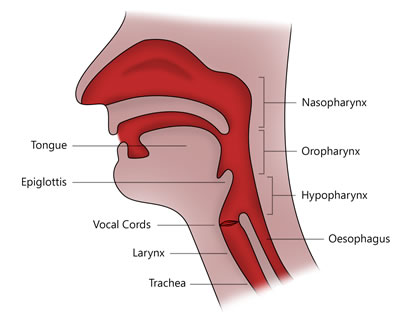
Nasopharynx
The beginning of the respiratory tract (the nasal cavity and oropharynx) is lined with moist mucous membranes. This lining is delicate and highly vascular. It deserves all the respect that you can give it, and that means preventing undue trauma by using liberally lubricated tubes and avoiding unnecessary poking about.
The nasal cavity is divided by a very vascular midline septum, and on the lateral walls of the nose are “shelves” called the turbinates. These projections can get in the way when tubes or other devices need to be inserted into the nostrils.
Oropharynx
The teeth are the first obstruction we meet in the oral part of the airway. They may be more obstructive in some patients than in others. The tongue is mostly a large chunk of muscle and represents the next potential obstruction. These muscles are attached to the jaw anteriorly and through a series of muscles and ligaments to the hyoid bone, a wishbone like structure just under the chin from which the cartilage skeleton (the larynx) of the upper airway is suspended.
The epiglottis is also connected to the hyoid, so elevating the hyoid will lift the epiglottis upward and open the airway further.
Hypopharynx
The epiglottis is one of the main anatomic landmarks in the airway. It looks like a floppy piece of cartilage covered by mucosa-which is exactly what it is-and it feels like the tragus- the cartilage at the opening of the car canal.
The epiglottis is attached to the hyoid and thence to the mandible by a series of ligaments and muscles. In the unconscious patient, the tongue can produce some airway obstruction by falling back against the soft palate and even the posterior pharyngeal wall.
However, it is the epiglottis that will produce complete airway obstruction in the supine unconscious patient whose jaw is relaxed and whose head and neck are in the neutral position. In such patients, the epiglottis will fall down against the glottic opening and prevent ventilation.
Larynx
The vocal cords arc protected by the thyroid cartilage, a boxlike structure shaped like a “C,” with the open part of the “‘c” representing its posterior wall, which is covered with muscle. In some patients, the cords can close entirely in laryngospasm, producing complete airway obstruction. The thyroid cartilage can easily be seen in most people on the anterior surface of the neck as the laryngeal prominence.
Inferior to the thyroid cartilage is another part of the larynx, the cricoid, cartilage shaped like a signet ring with the ring in front and the signet behind. It can be palpated as a small bump on the anterior surface of the neck.
Trachea
The tracheal rings (C-shaped supports for the trachea) continue beyond the cricoid cartilage, and the trachea soon divides into the left and right mainstream bronchi.
The point at which the trachea divides is called the carina. lt is important to note that the right mainstem bronchus takes off at an angle that is slightly more in line with the trachea. As a result, foreign bodies usually end up in the right mainstem bronchus.